Introduction
The treatment of choice for early-stage non-small cell lung cancer (NSCLC) is anatomical surgical resection. However, a growing number of patients are considered medically or functionally not amenable with surgery, also as a consequence of the progressively increasing age of the general population. In the past, a consistent proportion of these patients were not offered any kind of treatment or, in alternative, they underwent conventionally fractionated radiotherapy (RT), although with a considerably worse outcome if compared to surgical resection [1]. For stage I NSCLC, surgery is able to obtain survival projections at 12 years ranging between 69% (for tumors with a maximum diameter of 5-15 mm), and 43% (for larger tumors, with maximum diameter >45 mm). Conventional external beam radiotherapy is associated to 5-year overall survival (OS) rate of only 15%, with local failure rates ranging from 30% to 70% [2]. In the mid-1990s, at Karolinska Hospital in Sweden, researchers firstly transferred the principles of cranial stereotactic radiosurgery to extra-cranial tumor sites, especially lung [3]. This so-called stereotactic body radiotherapy (SBRT) approach, also known as stereotactic ablative radiotherapy (SABR), was then further developed by several centers worldwide [456]. SBRT is currently defined as a technique for delivering external beam radiotherapy with a high degree of accuracy to an extra-cranial target, using high doses per fraction, in 1-8 treatment fractions [7]. In the SBRT technique, specialized treatment planning results in high radiation dose with a steep dose gradient beyond the target; the challenge is to hit the entire extent of the tumor with an extremely efficient and biologically damaging therapy, while simultaneously avoiding the surrounding normal tissues (local tumor control rates of 90% and higher, with rates of severe toxicity below 10%).
SBRT for Medically Inoperable Non-Small Cell Lung Cancer
National Comprehensive Cancer Network Guidelines as well as the European Society of Medical Oncology (ESMO) Clinical Practice Guidelines now consider SBRT as the first line treatment option for medically inoperable patients affected with stage I NSCLC [7]. SBRT is an attractive alternative therapy for several reasons: outpatient, non-invasive, 20-30 minutes per treatment, short overall treatment time (1-2 weeks), no sedation or anesthesia (painless), immediate return to activities.
Population-based analyses from the Netherlands [89] and the United States [10] demonstrated an improvement in OS for stage I NSCLC in elderly patients following the introduction of SBRT in clinical practice. Haasbeek et al. [8] showed that for patients treated with radiotherapy OS was improved from 16 months to 24 months between 2001 and 2009 in the Netherlands. According to the data collected in the Amsterdam Cancer Registry, Palma et al. [9] demonstrated changes in treatment and survival in elderly patients with stage I NSCLC after the introduction of SBRT; in particular, a 16% absolute increase in RT use, a decline of 12% in the proportion of untreated elderly patients, and an improvement in OS.
Shirvani et al. [10] compared the effectiveness of lobectomy, sublobar resection, conventional radiotherapy, SBRT, and observation in patients older than 65 years, based on Surveillance Epidemiology and End Results (SEER) program. In this study, OS was significantly improved with SBRT and was similar to that after lobectomy.
Moreover, Hayashi et al. [11] retrospectively analyzed the clinical outcomes and feasibility in a series of 20 very elderly patients (age ≥85 years) with stage I NSCLC and 61 younger patients (age <85 years), demonstrating no differences in tumor control according to age, although very elderly patients experienced more frequently severe radiation pneumonitis (G3 pneumonitis in 10% and 0%, respectively).
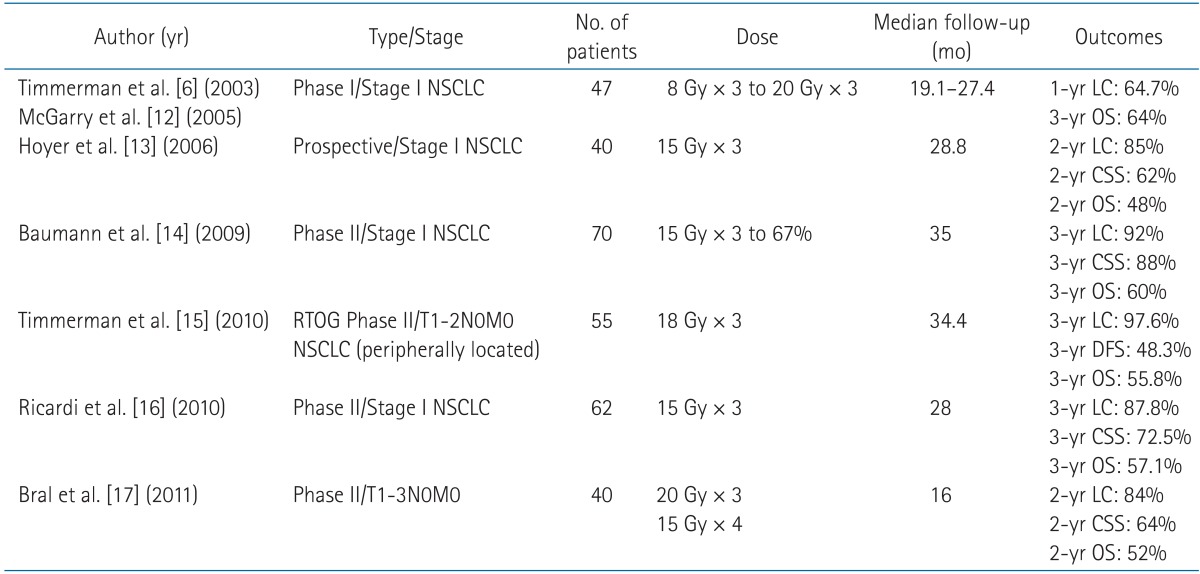
A part from retrospective, observational and registry studies, as shown in Table 1 several research groups have reported phase I and II trials of SBRT for early-stage NSCLC [6121314151617]. Total doses ranged from 45 to 66 Gy delivered in 3 or 4 fractions, with 2-3 years local tumor control rates and 1-3 years OS projections ranging between 84%-98% and 43%-72%, respectively. Timmerman et al. [6] and McGarry et al. [12] enrolled 47 patients between 2000 and 2003 in one of the first phase I studies to evaluate the safety of SBRT in clinical stage T1 or T2 tumors, lymph node negative, medically inoperable NSCLC [13]. The initial dose was 24 Gy over 3 fractions, then escalated by 2 Gy per fraction increments up to the total dose of 60 Gy. With 60% of partial response rate and 27% of complete response rate, mean tolerated dose was not reached for T1 tumors, though for tumors >5 cm, the mean tolerated dose was determined to be 66 Gy. In the United States, preliminary interesting findings from the University of Indiana led to the design of the Radiation Therapy Oncology Group (RTOG) 0236 trial, a phase II study in which 55 patients were enrolled and all received 60 Gy in 3 fractions for peripherally located tumors. Results demonstrated a 3-year actuarial local control (LC) rate of 98%, with OS at 3 years of 56% (median OS of 4 years) [15].
As better local tumor control was shown to go along with higher OS in patients treated with conventional radiation therapy [18], it can also be expected that improvements in local control and survival can be achievable by applying higher SBRT doses [10]. To help better define the dose and fractionation required for tumor sterilization with SBRT, various studies examined the biologically effective dose (BED) delivered to the tumor. In a Japanese multi-institutional retrospective review of 245 patients treated with a variety of dose and fractionation schedules, Onishi et al. [19] concluded that local control was significantly improved with BED greater than 100 Gy (prescription dose at isocenter), with 5-year LC rate of 84% for BED10 > 100 Gy vs. 37% for BED10 < 100 Gy (p < 0.001). More recently, Kestin et al. [20] found a significant correlation between BED10 > 105 Gy (prescription to the edge of the PTV, with 60%-90% of the isocenter dose) and higher local control. A meta-analysis done by Zhang et al. [21] evaluated the optimal BED by analyzing 34 previously reported studies. After dividing the studies into subgroups based on the BED quartiles (low, medium, medium-high, and high), they showed that the outcome got worse for BED below 83.2 Gy and for BED exceeding 146 Gy. In 2015, researchers from the University of Illinois at Chicago, examined different SBRT dose schedules using the National Cancer Database and found that patients with T2 tumors treated with a BED10 > 150 Gy (roughly equal to 54 Gy in 3 fractions) had a significantly improved survival compared with patients treated with a BED10 < 150 Gy [22]. Nowadays, the current recommended dose for SBRT is a minimum of 100 Gy BED, prescribed to the target volume encompassing isodose, typically delivered in one to eight fractions.
As fatal toxicities were previously reported when treating central tumors (in close proximity of critical structures such as main bronchi, trachea and big vessels) [23], subsequent studies showed that the use of 'risk-adapted' fractionation schemes delivering the minimal required dose of 100 Gy BED in a larger number of fractions were able to obtain satisfactory tumor control rates with an acceptable toxicity [24].
Large retrospective observational studies confirmed the good results described above in clinical practice. The working group 'Extra-cranial Stereotactic Radiotherapy' of the German Society for Radiation Oncology (DEGRO) conducted a multicenter study on patterns of care and outcome analysis on a cohort of 582 patients treated with SBRT in Germany and Austria between 1998 and 2011. In this study, dose escalation (BED of at least 106 Gy) emerged as significant factor influencing OS and LC, while stage IA was correlated with a better OS, with only a trend for a better LC [25]. Similarly, in a cohort of 196 patients with histological/cytological diagnosis of NSCLC treated with SBRT included in an Italian multicenter observational study, stage IA was correlated with better OS and cancer-specific survival (CSS) [26].
The pattern of relapse following SBRT is characterized by a predominant failure at distant sites, with a significant impact on OS (together with non-cancer deaths secondary to other comorbidities typical of an elderly non-surgical population). The probability of distant metastases is up to 20%-26% of cases and is related to tumor size [25262728].
Despite the difficulties in conducting randomized clinical trials (RCTs) comparing SBRT with surgery or conventional radiotherapy, at the European Society for Radiotherapy and Oncology (ESTRO) 2014 meeting, the results of the SPACE trial were presented in abstract form [29]. This trial randomized 102 patients to SBRT (66 Gy in 3 fractions and 45 Gy at the periphery) or conventional radiotherapy (70 Gy in 35 fractions); with a limited follow-up, local control did not differ between the two arms, but the conventional treatment was associated with a higher risk of grade 1-2 toxicity (esophagitis and pneumonitis). Accrual to a similarly designed RCT (CHISEL, Clinicaltrials.gov NCT01014130) is ongoing; however, unlike SPACE, CHISEL employs smaller margins and cone beam computed tomography (CT) setup in the conventional RT arm.
SBRT for Medically Operable Patients
Standard therapy for operable, clinical stage I, NSCLC is lobectomy with mediastinal lymph nodes sampling [30]. Today, sublobar anatomical resection (segmentectomy) is discussed as another possible option [31], but comparative studies between segmentectomy and lobectomy are still ongoing [32].
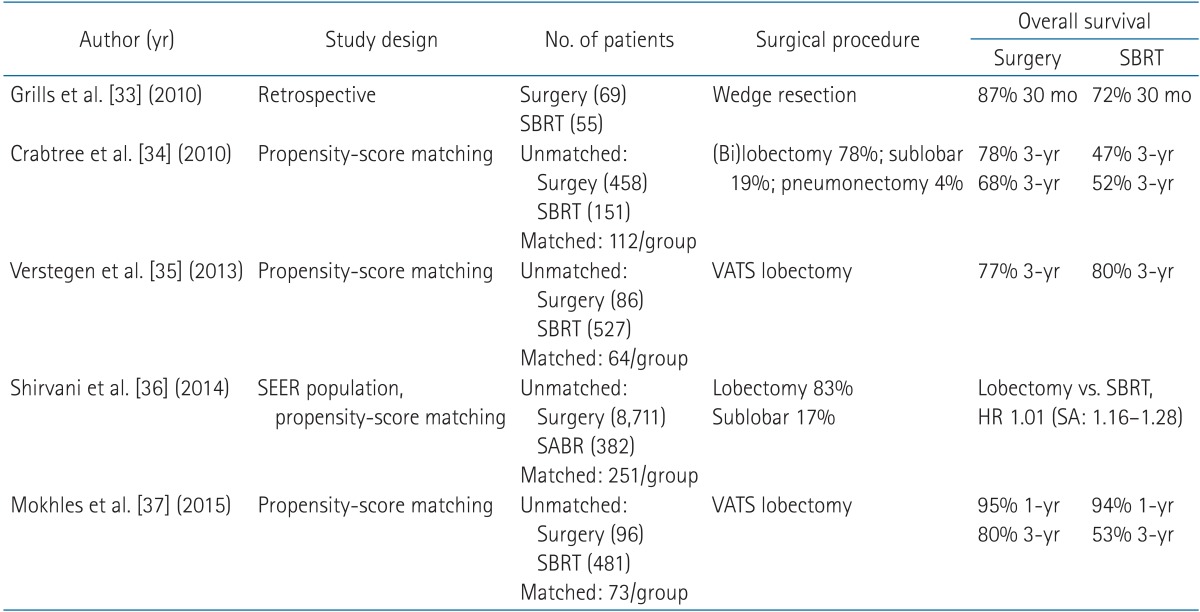
As summarized in Table 2, findings from population-based studies and propensity score matched analyses suggest that overall survival and disease-specific survival after SBRT are similar to those after surgery [3334353637]. However, concerns remain about the risk of local or nodal recurrence after SBRT, either of which could lead to worse OS. Grills et al. [33] performed a retrospective single-institution comparison between SBRT and wedge resection, showing improved local tumor control in favor of SBRT (5% vs. 24%), no differences in CSS and a superior OS projection for the surgical cohort (older age and increased comorbidities in the SBRT patients). Crabtree et al. [34] analyzed 257 patients, again with the propensity score method, and demonstrated no difference between local recurrence, CSS or OS after 3 years between SBRT and surgery. Verstegen et al. [35] compared SBRT and video-assisted thoracoscopic surgery (VATS) lobectomy in 128 patients after matching for patients' characteristics (as gender, age, performance status, clinical tumor stage, location of the tumor, tumor histology, forced expiratory volume in the first second [FEV1], and Charlson comorbidity index). Locoregional control resulted to be better after SBRT, with no differences in freedom from progression and OS. The previously cited US population-based SEER analysis found no difference in OS and CSS for SBRT versus sublobar resection or lobectomy after propensity score matching [36]. Recently, Mokhles et al. [37] selected 577 patients (96 who undergone VATS or open lobectomy at Erasmus University Medical Center of Rotterdam and 481 treated with SBRT at Vrije University Medical Center in Amsterdam) and matched two cohorts of 73 patients in each group, according to propensity score method. OS rates at 12 and 60 months were 95% and 80% in surgery group, and 94% and 53% in SBRT group, respectively (p = 0.089). This trend towards an improved survival after 3 years in surgically treated patients could be explained by the pathological lymph node staging (selection of patients requiring adjuvant therapy), and by differences between the two groups, as the matching was done with only a limited number of variables (i.e., staging procedure was not included as a covariate). Long-term follow-up SBRT studies are needed to fully confirm this finding.
Few studies (with limited numbers of patients) reported the outcomes after SBRT in patients who refused surgery, reporting 3- and 5-year OS rates higher than 80% and 70%, respectively [3839].
Three phase III randomized studies have been initiated to compare SBRT with surgery in patients with early-stage NSCLC (the STARS trial [NCT00840749], the ROSEL trial [NCT00687986], and the ACOSOG Z4099 trial [NCT01336894]), but they were all closed earlier because of the slow accrual.
In May 2015, a pooled analysis of the data from STARS and ROSEL trials (that had similar entry criteria) has been published [40]. Overall, 58 patients were enrolled and randomly assigned (31 to SABR and 27 to surgery); with a median follow-up of 40.2 months for the SBRT group and 35.4 months for the surgery group, OS at 3 years was 95% and 79% (HR, 0.14), respectively. Three patients (10%) in the radiotherapy group had grade 3 treatment-related adverse events, with no grade 4 or treatment-related deaths. In the surgery group, one patient (4%) died of surgical complications and 12 patients (44%) had grade 3-4 treatment-related adverse events.
Toxicity and Quality of Life
Radiation pneumonitis (RP) is one of the most common toxicities after SBRT, as well as after conventional radiotherapy to the lung. Most of the RP is of grade 1 or 2 and either asymptomatic or manageable, but in few cases may be severe and symptomatic. In large retrospective studies, the incidence of grade ≥2 RP was below 8% [2541]; a higher incidence of severe RP has been reported only in patients with pre-existent idiopathic pulmonary fibrosis [42].
SBRT may be safely delivered in patients with severe pulmonary comorbidities and in patients with very poor pre-treatment pulmonary function. Previous retrospective studies analyzed changes in pulmonary function test (PFT) following SBRT, with variable follow-up intervals: most of them were limited to spirometric parameters and diffusing capacity for carbon monoxide (diffusion capacity of lung for carbon monoxide [DLCO]). Guckenberger et al. [43] reported that there was no association between pre-treatment PFT values and the incidence of RP in patients with severe chronic obstructive pulmonary disease (COPD) globally initiative for chronic obstructive lung disease (GOLD) stage III-IV, with a loss of <10% (FEV1, DLCO) within 24 months after treatment. Recently, a more comprehensive analysis of 'complete' PFTs (including blood gas analysis) was reported, on a series of patients enrolled in the RTOG 0236 phase II trial [44]. In this report, including the data of 55 patients followed over a 2-year interval, the mean percentage in FEV1 and DLCO decline were 5.8% and 6.3%, respectively, with minimal changes in blood gases and no significant decline in oxygen saturation. The authors concluded that no clinically significant changes in pulmonary function were evident after SBRT, at a dose of 54 Gy in 3 fractions.
The few studies describing quality-of-life (QoL) after SBRT have limited follow-up and analyzed patients less fit at baseline, reporting that SBRT had no detrimental or negative on QoL. In general, overall QoL as well as the subdomains of dyspnea and cough, was stable after SBRT [45].
Rib fractures and neuralgia have been reported in few patients, when tumor was close to chest wall. Severe toxicity to the brachial plexus (neuropathic pain, motor weakness, or sensory alteration), large bronchi (stenosis with pulmonary atelectasis), and esophagus (ulceration, perforation, fistula) has been reported but these events are uncommon.
There have been few studies on CT findings after SBRT for lung cancer, describing two stages: early acute RP that occurs within 6 months of treatment and radiation fibrosis that occurs 6 months or more after treatment. CT findings after SBRT does not seem to have the same appearance, distribution and progression as those following conventional radiotherapy; this is due to the difference in dose delivery, biologic effects and overall treatment time. In order to provide useful evaluation systems of radiological changes after SBRT, researchers developed different scales using descriptive categories. Acute radiological toxicity was scored using a five-point scoring system developed by Vrije University [46], modified from Kimura et al. [47] (1, diffuse consolidation; 2, patchy consolidation; 3, diffuse 'ground glass opacity'; 4, patchy 'ground glass opacity'; 5, no changes). Late radiological toxicity was scored according to the Koenig's Scale (0, absence of changes; 1, modified conventional pattern; 2, mass like pattern; 3, scar like pattern) [48]. Radiation-induced lung injury can manifest as a CT-density changes in up to 90% of cases at 2 years after SBRT. These changes can occasionally mimic a tumor recurrence; therefore, it is important to recognize some high-risk radiological features on serial CT scans that are suggestive of recurrence (i.e., enlarging opacity, sequential enlargement, enlargement after 12 months, bulging margin, linear margin disappearance, loss air bronchogram, and craniocaudal growth) [49].
Technical Aspects
Several professional groups have reported guidelines for SBRT, and technological advances together with dedicated quality assurance programs have improved the ability of radiation oncologists to deliver large hypo-fractionated doses. SBRT can be performed using either traditional linear accelerators (equipped with image-guidance technology) or linear accelerators specifically adapted for SBRT with dedicated delivery systems. The SBRT procedure was initially defined by the use of stereotactic frame-based patient set-up. Currently, in many centers a frame-based patient set-up has been replaced by image-guidance (frameless SBRT). With frameless patient set-up, external stereotactic coordinates are replaced by the visualization of a patient's anatomy by using images acquired on-table and subsequently compared with pretreatment planning images. Several technologies for image guidance are commercially available, and superiority of one method over the other has not been demonstrated. Use of volumetric imaging (cone beam CT), as opposed to only implanted fiducials, has the advantage of enabling assessment of changes in target shape and position, relative to the position of organs at risk.
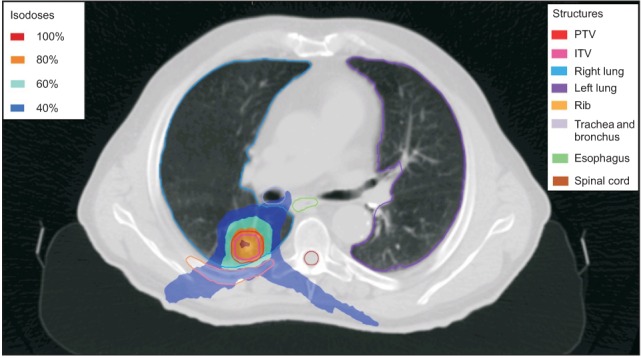
Four-dimensional CT is the recommended technique for SBRT simulation, due to its ability to accurately compensate for target motion and to define patient's specific internal margins. For planning, all published prospective trials have used three-dimensional conformal treatment planning, but more recently, also intensity-modulated radiation therapy (IMRT) and advanced rotational techniques, such as volumetric modulated arc therapy (VMAT), have been widely adopted. VMAT is a form of IMRT in which the gantry continuously moves around the patient with a varying speed and rate of dose delivery. The maximal dose rate reachable by some linear accelerators, with a flattening filter free technique, is up to four times faster than the standard. Fig. 1 illustrated a typical VMAT plan in a man of 78 years old, affected by a peripheral NSCLC in stage IA (cT1aN0M0). When using IMRT planning, larger volumes of normal pulmonary tissue, including contralateral lung, can be exposed to low radiation doses (V5); especially when treating larger tumors, doses to the contralateral lung may predict for the risk of pneumonitis [50]. However, a publication showed no difference in the incidence of radiation pneumonitis between three-dimensional conformal radiation therapy (3D-CRT) and VMAT [47].
Regarding delivery phase and active motion management strategies, continuous irradiation in free breathing is performed using the internal target volume concept, the mean target position concept, or real-time tumor tracking. Non-continuous irradiation of the tumor in a reproducible position is performed using gated beam delivery in predefined phases of the breathing cycle.
Conclusions
Approximately 25% of patients affected with stage I NSCLC are not eligible for surgery due to medical contraindications. For these patients, SBRT is currently considered the best alternative option, on the basis of the previously mentioned prospective and retrospective studies. Even for centrally located tumours and for patients with poor pulmonary function, SBRT has been shown to be feasible and efficient. Toxicity is generally mild, with most of the patients developing late radiological toxicity without a serious impairment of the lung function over time. The recently reported retrospective studies comparing SBRT versus surgery added important information to the evidence accumulated in the first decade of SBRT use. Moreover, the prospective comparison between SBRT and lobectomy in operable patients obtained by merging the ROSEL and the STARS phase III trials suggested a substantial equivalence between surgery and radiotherapy, with perhaps a better outcome in terms of survival for SBRT due to the virtual absence of treatment-related mortality, which is higher for lobectomy (both open and video-assisted). At the same time, the few retrospective studies that compared limited surgery (segmentectomy or wedge resection) vs. SBRT were generally in favour of SBRT, with results of difficult interpretation. It should be noted that all these retrospective comparisons suffer from several intrinsic limitations and flaws. The most important are that, albeit the analyses were all adjusted for risk factors, biases in patients' selection could not be completely avoided, suggesting an indication but not clear evidence in favour of one treatment modality over the other. One of the most important issues is the median follow-up time of the treated cohorts: for SBRT is generally shorter, and this may have an impact in evaluating survival projections after 3 years, as underlined by one of the cited studies [36] where, surprisingly, the survival rates after 3 years were clearly superior for surgery.
In conclusion, available evidence suggests that SBRT is an efficient and safe therapy for stage I inoperable NSCLC patients; being better tolerated than surgery, SBRT might also be considered a valid therapeutic option for operable patients. In clinical practice, a multidisciplinary approach should be implemented with the aim of determining the best treatment strategy on an individual basis. In the decision process, many factors should be taken into account, like respiratory function, tumor's dimension and location, age, comorbidities and patient's preference, with the goal to offer the proper therapeutic choice in terms of efficacy and morbidity.