Introduction
Post-operative radiation therapy is the common treatment of breast cancer, which can reduce the locoregional recurrent rate. Breast cancer is a common challenge in radiotherapy due to a variety of treatment conditions. Many techniques are applied, such as intensity-modulated radiation therapy or volumetric modulated radiation therapy used for bilateral breast irradiation [1], breathing controlled used for left side breast irradiation. However, breast irradiation treatment usually consists of medial and tangential beams designed to reduce radiation dose to the underlying heart and healthy lung tissue [2]. Patient immobilization in conjunction with treatment planning is essential to reduce the irradiated volume of the healthy tissues. Especially for the left breast irradiation, a low dose of radiation may induce the late complication to the heart such as the morbidity and mortality, even though the complication may also arise from other factors, such as systemic treatment and patient’s comorbidities [3]. Many studies reported the radiation dose to the heart on left breast irradiation [4-6].
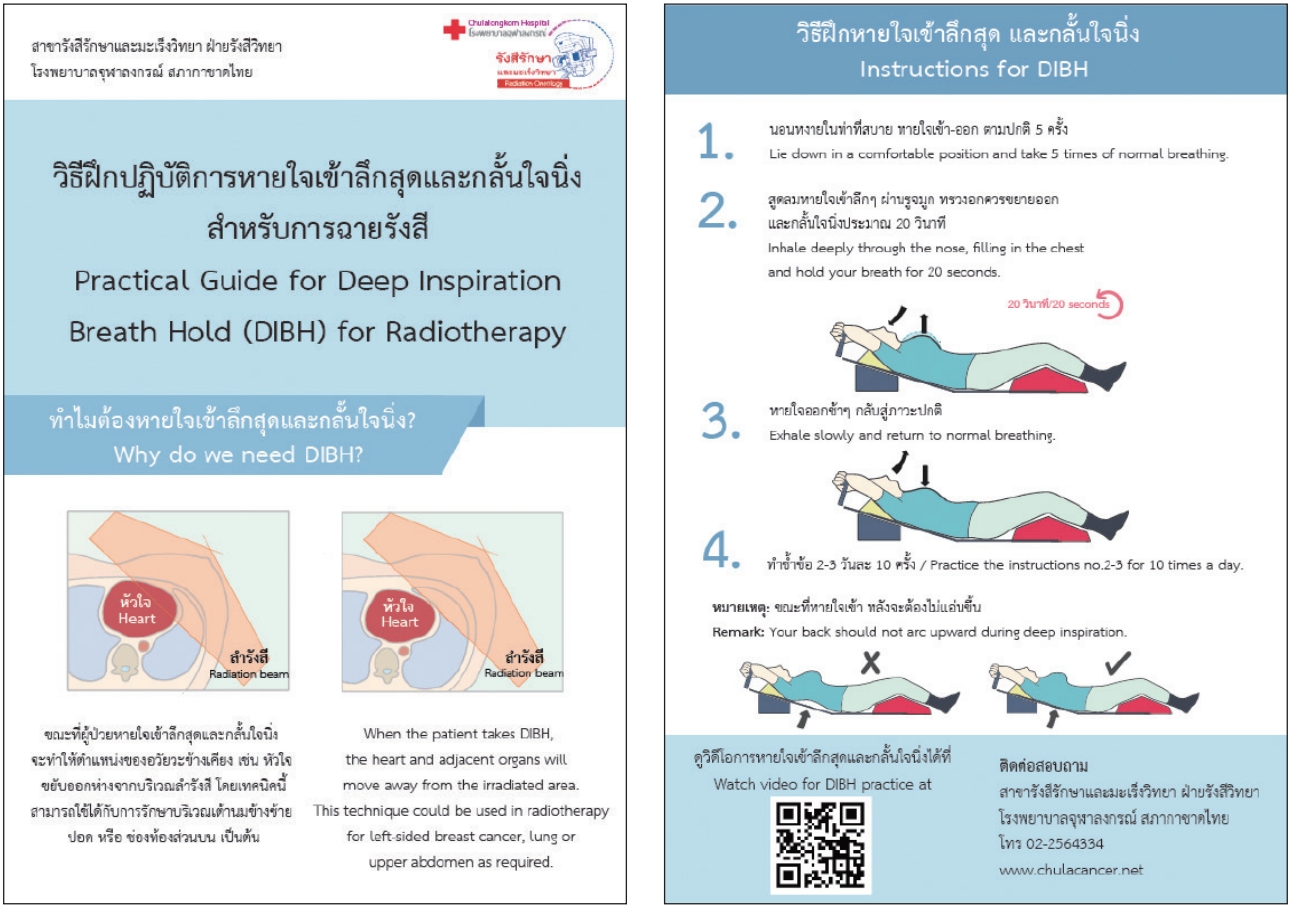
One of the advanced treatment techniques which are more sophisticated to reduce the radiation dose to the heart is deep inspiration breath hold (DIBH) technique. Several of the literature confirmed that this technique could reduce the radiation dose to the heart [5-14] and lungs [10,13,15-18] during left beast irradiation. For the DIBH technique, patients should take deep inspiration and hold for approximately 20 seconds during the simulation or treatment process. The air filling inside the chest will move the heart position away from the treatment field. This technique will gain success once the patient completes the breath hold compliance. Motion management training is essential preparation for this group of patient. Our center has started treating patients with DIBH technique since 2015. The tools that used to track the breath hold position during the simulation process was the RPM marker block while a 3D surface imaging system (AlignRT; Vision RT Ltd., London, UK) was used to track the real-time patient position in treatment delivery.
The main problem which deteriorates the success of DIBH procedure is the patient’s pressure during the simulation. The training session takes around 20–30 minutes, which is tedious yet making patients stress and uncomfortable. Although radiation oncologists have explained to patients about the information on DIBH technique before the treatment, defects still probably occur and generate a serious problem, for example, the unclear detail in the patient’s body. We initiated the idea to create an information sheet, so patients can learn the DIBH in detail and train themselves before the simulation starts. Not only the instruction sheet but also the tutorial video that depicts the process of simulation for DIBH patient were created. This document was handed to the patient one week before the simulation session. For the video, it can be easily accessed via our department website (http://www.chulacancer.net), QR code scanning, or browsing via Google or Youtube.
This article reviewed the success of implementing the instruction sheet and educational video for patients who underwent radiation treatment with DIBH technique. The feasibility and efficacy of the guidelines were evaluated based on the simulation time, started from a patient lying down on the couch until image acquisition was completed. The laborious time during computed tomography (CT) simulation process declined when patients obeyed the practical guidelines.
Materials and Methods
The patients with left breast cancer who underwent DIBH procedure from October 2017 to August 2018 were observed. The patients were divided into four groups: group A is the patients who did not treat with DIBH technique, group B is the DIBH patients without instruction material (before the instruction sheet and educational video launched), group C is the DIBH patients with instruction material via instruction sheet or educational video, and group D is the DIBH patients with instruction material for both sheet and video. The group C and D patients, the data collected after the instruction sheet and educational video were launched. To avoid unwanted bias results, the patients of group C and D were not assigned or suggested any instruction materials for them, but they can select the preferable methods. The selected materials from patients were confirmed again via remarkable items on the questionnaire.
The information sheet comprised of the aim of DIBH technique, step by step for practice, figures, and the QR code to access the 3-minute educational video, where patients can directly follow its instructions. This guideline was given at least 1 week before the simulation started. Both Thai and English languages were provided. Fig. 1 shows the printed document on both sides on size A5 (5.8 x 8.3 inches).
On the simulation date, patients must fill up the questionnaire regarding their satisfaction of both document and video before the CT simulation started. The questionnaire consists of two parts. The first part composes of the personal history of the patient, such as age, patient’s education group, the experience of radiotherapy, and the information on the DIBH technique. The second part is the level of satisfaction, which categorized into five levels: extremely satisfied, very satisfied, moderately satisfied, dissatisfied, and extremely dissatisfied. Those levels were represented by score 5, 4, 3, 2, and 1 for each level, respectively. We explained to patients that the questionnaire did not influence the treatment process.
The Philips Brilliance Big Bore 16-slice and Siemens SOMATOM Definition AS 64-slice CT simulation were utilized in our department. The patient position was supine, and both hands were raised overhead. The breast board (CIVCO Medical Solutions, Orange City, IA, USA) was used for immobilization. The Varian real-time position management (RPM, Varian Medical System, Palo Alto, CA, USA) observed the breath-hold level from the respiratory curve at CT simulation. The simulation time process was observed from patient positioning until completion of CT scanning. The images data set was acquired in the free breath and DIBH technique for all cases. The range of scanning covered the ears to L2 with 3 mm of slice thickness.
Results
The total of 112 cases was analyzed; 92.6% of these patients never had an experience in radiotherapy before. There was no significant difference among the average age of patients for all groups as depicted in Table 1. The simulation time for DIBH cases which was categorized into four groups is listed in Table 1.
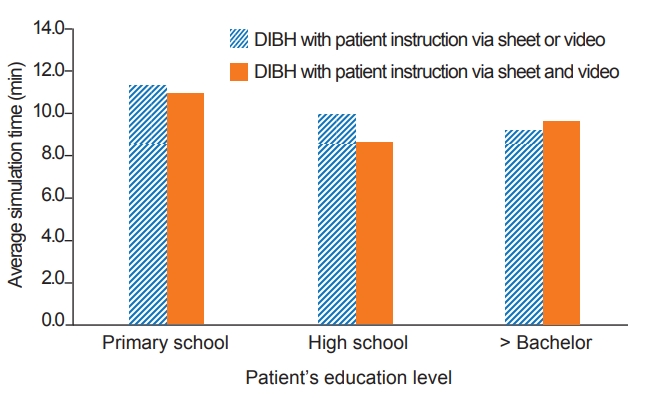
The simulation time reduced significantly when the patient followed the practical guidelines. However, the difference was not significant between the DIBH with instruction materials via sheet or video or using both of them. It could imply that either the instruction sheet or video was enough depending on the patient’s preference.
The satisfaction scoring parameters of the questionnaire were evaluated for the practical guide document and the video as can be seen in Table 2. All parameters showed an excellent level, 4.6 ± 0.1 and 4.5 ± 0.1 for document and video, respectively.
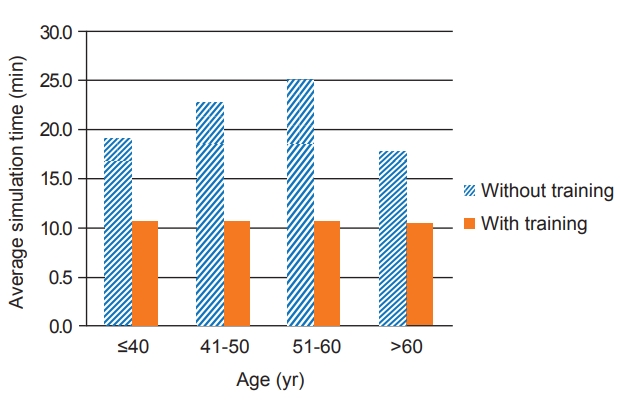
The coaching strategy for DIBH patients is essential. Many factors are affecting the success in the process—for instance, age, voluntary, the condition of patients, etc. [19]. This study did not limit the patient’s age for the DIBH technique. However, radiation oncologist observed patient’s status by physical observation such as the patient who can cooperate in the DIBH training or who do not have any respiratory function impairment. Relationship between patient’s age and simulation time was explored in Fig. 2. The average simulation time was reduced significantly after training for all range of the age. Nevertheless, there was no significant difference in simulation time among the group of age after training. This result indicated that the instruction sheet and educational video for DIBH training could be employed within all range of patient’s age. The threshold point of patient’s age for non-beneficial of DIBH is still unambiguous in this study. Czeremszynska et al. [19] supported that the age alone cannot be appointed as a criteria for the DIBH technique.
The average simulation time and patient’s education relationship was shown in Fig. 3. For each patient’s education group, there was no significant difference in the average simulation time (p > 0.05) for patients who used the instruction sheet or video alone, or used both of them for all groups. The simulation time was comparable between the group of the patient’s education with no significantly different (p > 0.05).
The treatment time of DIBH training is out of the scope of this study since different modality was used in breath hold monitor. The real-time 3D surface imaging system (AlignRT) equipped on the linear accelerator was utilized for setup verification in the delivery process while the Varian real-time position management (RPM) was used in CT simulation.
Discussion and Conclusion
The instruction materials confirmed its efficacy to save the simulation time. It does not mean save only time itself, but also implicitly increase the cost-effectiveness because the staff workload decreased and was not considered as burden for patients. Decreasing the workload may increase the number of patients on the simulation procedure. In addition, it also could reduce their waiting time.
The patient coaching before simulation could potentially reduce the lengthy time on the simulation process for DIBH technique. The different outcome of patient compliance using either instruction sheet or video or both of them were not significant. This study encourages patients to practice the DIBH technique properly as it can enhance the success of left-sided breast treatment.