Long-term toxicities after allogeneic hematopoietic stem cell transplantation with or without total body irradiation: a population-based study in Korea
Article information

Abstract
Purpose
To compare long-term toxicity incidences, including secondary cancer (SC) with or without total body irradiation (TBI), in Asian patients receiving allogeneic hematopoietic stem cell transplantation (HSCT) using a nationwide database.
Materials and Methods
We identified 4,554 patients receiving HSCT for leukemic disease from 2009 to 2016 using the healthcare bigdata system of Korea. Incidence rate ratios (IRRs) for SC, cataracts, hypothyroidism, chronic kidney disease (CKD), myocardial infarction, or strokes were compared, and standardized incidence ratios (SIR) of SC was also estimated.
Results
TBI was conducted on 1,409 patients (30.9%). No overall survival differences based on TBI were observed. With a median follow-up duration of 58.2 months, 143 patients were diagnosed with subsequent SC (3.4%). Incidence rates per 1,000 person-year were 6.56 (95% confidence interval [CI], 4.8–8.8) and 7.23 (95% CI, 5.9–8.8) in the TBI and no-TBI groups, respectively (p = 0.594). Also, the SIR (95% CI) was not significantly increased by TBI (1.32 [0.86–1.94] vs. 1.39 [1.08–1.77] in the no-TBI group). In the young age group (0–19 years), SIRs were increased in both groups regardless of TBI (8.60 vs. 11.96). The IRRs of cataracts (1.60; 95% CI, 1.3–2.0), CKD (1.85; 95% CI, 1.3–2.6), and hypothyroidism (1.50; 95% CI, 1.1–2.1) were significantly increased after TBI. However, there were no significant differences in the occurrence of myocardial infarction and stroke according to TBI.
Conclusion
Our results suggest that modern TBI may not additionally increase the risk of SC after allogeneic HSCT, although increased risks of other diseases were noted. Physicians should carefully consider individualized risks and benefits of TBI, with a particular focus by age group.
Introduction
Traditionally, total body irradiation (TBI) has played an important role as a conditioning regimen in situations in which hematopoietic stem cell transplantation (HSCT) is required to treat various leukemic diseases [1]. The reasons for reconsidering or excluding TBI in the treatment decision-making process are concerns about potential toxicities after TBI, such as growth retardation and secondary cancer (SC), especially in pediatric patients [2,3]. Theoretically, there may also be toxicities due to functional deterioration of exposed organs, but these are not easy to study comprehensively; thus, there are few related reports. It is difficult to collect the occurrence data of long-term toxicities due to limitations in patient follow-up with data from a single or small number of institutions. In particular, observational studies on long-term toxicity or health status after TBI in Asian patients are very limited. Some previous studies have only focused on graft-versus-host disease, disease recurrence, and death [4,5].
In Western population, numerous reports have been published on the long-term therapeutic toxicity of TBI. Researchers at Washington University reported a cumulative incidence rate of 22% for SC up to 30 years after transplantation, based on an analysis of 4,905 patients who underwent TBI between 1969 and 2014 [6]. However, a study conducted at the Detroit Medical Center reported a significant cumulative incidence of cataracts (16%), while only two cases (0.3%) of SC were observed following TBI [7]. The discrepancy in the above results seem to reflect the differences in treatment periods for included patients and changes in treatment paradigms, such as the development of general supportive treatment and the increased use of low-intensity TBI-containing regimens. However, there are also many limitations of retrospective studies conducted at single institutions, and it is difficult to draw consistent conclusions about the long-term health effects of TBI. Until now, the incidence of SC after TBI has not been clearly identified, and more large-scale studies are needed. Furthermore, there is still a lack of large-scale patient outcomes data for various potential organ toxicities such as chronic kidney disease (CKD), hypothyroidism, myocardial infarctions (MI), or strokes. Specifically, there is scarce data regarding these in the Asian population and racial differences make it difficult to extrapolate from Western data.
In the modern era, with the increasing number of long-term survivors after HSCT, it is crucial to identify strategies that effectively reduce or prevent side effects that directly impact patients' long-term quality of life. A comprehensive understanding and observation of the long-term health effects associated with each treatment are necessary. Fortunately, Korea's nationwide medical insurance system facilitates large-scale research at a national level, allowing for numerous studies on various diseases [8,9]. Moreover, the aforementioned diseases (SC, cataracts, CKD, hypothyroidism, MI, or stroke) require physicians to record them in the database to ensure coverage of related prescriptions or procedures by national insurance. This enables the frequency of occurrence to be captured relatively accurately even in a large national-level patient group. Therefore, we aimed to compare the incidences of possible long-term toxicities with or without TBI in Asian patients receiving allogeneic HSCT using the large-scale national population-based database.
Materials and Methods
1. Establishment of study cohort and variable definition
We performed this work using the healthcare bigdata system proved by the Health Insurance Review and Assessment Service (HIRA) of the Republic of Korea. Since almost every citizen (97%) is covered in the single public medical insurance system, the insurance claim database represents medical practice in South Korea and includes information on diagnoses, prescriptions, treatments, and treatment results, such as death [10]. After obtaining the approval of Seoul Metropolitan Government–Seoul National University Boramae Medical Center (No. 07-2022-16) and HIRA (No. M20220405920), we established the customized database of all 4,682 patients who underwent HSCT for leukemic disease (ICD-10 codes, C91–C95) from 2009–2016. All claim data were downloaded from 2007, when the database was first available, to ensure a wash-out period of at least 2 years from the date of HSCT (index date, denoted as iDate) and follow-up data were reviewed until 2021. Patients with previous diagnoses of other malignancies or transplantation histories (solid organ or HSCT) were excluded; 4,554 patients were included in the main analysis.
From the hospitalization claims for HSCT, conditioning chemotherapy (CTx) and TBI were extracted using billing and procedure codes. To evaluate the comorbidities of each patient, we calculated the Charlson Comorbidity Index (CCI) using the diagnosis codes in the administrative database within 1 year from the iDate [11]. Long-term toxicities following HSCT were defined as follows: (1) SC, defined as at least one new diagnosis of subsequent second primary malignancy, except for leukemia, in the hospitalization database; (2) cataract, with cataract surgery codes [12] in patients without previous histories of cataracts; (3) hypothyroidism, with new drug prescriptions (levothyroxine, liothyronine, or combined agents) 90 days or more after HSCT; and (4) newly diagnosed CKD, MI, or stroke after HSCT defined as a previous publication [13]. In patients under 20 years, somatropin treatment was defined as somatropin injection treatment over three times or more.
2. Statistical analysis
The χ2 and Student t-tests were used to compare categorical variables and continuous variables between groups, respectively. The follow-up duration for each endpoint was calculated from the iDate to the occurrence date of each defined event, as aforementioned, or the last follow-up date (September 30, 2021; last claim data provided). Survival analysis was performed to estimate the occurrence of long-term toxicity or overall survival (OS) using Kaplan–Meier method, and patients who died early after HSCT were excluded from the analysis to eliminate the impact of treatment-related mortality (TRM), which was defined as any cause of death within the first 90 days following HSCT. The impact of clinical variable on survival was assessed by log-rank tests in univariate analysis and Cox proportional hazard model in multivariate analysis, respectively. Due to the nature of the retrospective study, meaningful characteristic differences between groups based on TBI were observed. Thus, we performed a propensity-score matching (PSM) analysis also to adjust for imbalances in patient characteristics in the groups organized according to the administration of TBI using the nearest method and calipers of width 0.2. After PSM, we examined the imbalance between groups using the standardized mean difference (<0.1 means the resolution of imbalance).
A crude rate was calculated by dividing the number of patients with late-term toxicities by the number of patients in the target group. To consider the number of people exposed and follow-up times, the incidence rate (IR) was calculated as the number of events per 1,000 person-year. The incidence rate ratio (IRR) was defined as the ratio of the IR of the exposure group to the IR of the non-exposure group to compare IRs between two groups. Each confidence interval (CI) of IR or IRR was estimated using the exact Poisson method.
The standardized incidence ratio (SIR) was estimated to determine whether the incidence of SC after HSCT was significantly increased compared with that of the general population. The Korean Statistical Information Service provides statistical information about cancer cases and incidence rates by sex, age, and year based on the National Cancer Registration and Statistics System [14]. Using these data, we calculated the SIR (observed/expected in the matched general population) and 95% CI adjusted for age, sex, and calendar year.
A p-value <0.05 was deemed statistically significant, and all statistical analyses were conducted using R version 3.5.1 (http://www.r-project.org).
Results
1. Patient characteristics
A total of 4,554 patients who met the inclusion criteria were included, and baseline characteristics are presented in Supplementary Table S1. The median age of the patient group was 41 years (interquartile range [IQR], 25 to 52 years), and 19.4% of patients were under 20 years of age. The CCI scores of patients were mostly 0–2 (77.1%), and 1,409 patients (30.9%) received TBI. In overall dataset receiving allogeneic HSCT, lymphoid leukemia (C91) accounted for 1,512 patients (33.2%), myeloid (C92) 2,510 patients (55.1%), and others (C93–C95) 342 patients (7.5%).
For pre-HSCT conditioning, busulfan/fludarabine (Bu/Flu) or Bu/Flu-containing regimens were the most commonly used in CTx-only settings (62.2%) and cyclophosphamide (Cy) or Cy-based regimens were most often used in combination with TBI (44.8%). The median follow-up duration was 58.2 months (IQR, 10.2 to 96.2 months).
A total of 266 patients died within 90 days after HSCT; therefore, the overall TRM was 5.8%. There was no significant difference in TRM whether TBI was administered or not (p = 0.260) (Supplementary Fig. S1A).
2. Overall survival analysis
Five-year OS was 59% in the study population, and the median survival had not been reached. Survival analysis indicated that the impact of age, sex, subtype, high CCI, and TBI on OS was significant after adjusting variables (Supplementary Fig. S1B, Supplementary Table S2).
However, there were significant imbalances in the baseline characteristics between patients in the TBI and no-TBI groups. TBI was performed more often in relatively young patients, patients with lymphoid leukemia, and those with more comorbidities. After PSM, most patient factors, except the conditioning regimen, which depends on TBI, were adjusted, leaving 1,273 patients in each group (Table 1). In the matched cohort, favorable survival was achieved in young or female patients and in patients with fewer comorbidities, but no survival difference according to TBI was observed (p = 0.432) (Supplementary Table S2).

Comparison of patient characteristics according to the receipt of total body irradiation before and after propensity-score matching
3. Cumulative incidence of SCs according to whether or not TBI was administered
Of the 4,258 patients who survived more than 90 days after HSCT, 143 patients were diagnosed with subsequent SCs (crude ratio of 3.4%). The most common cancer types were gastrointestinal cancers (C15–C26; 40 patients) followed by lymphomas (C81–C85; 32 patients) (Supplementary Table S3). The median interval from the iDate to SC diagnosis was 48.5 months. The distribution of intervals between HSCT and SCs occurrence varied depending on the SCs type; the longest intervals were for cancers of male genital organs (C64–C68; median of 83.8 months), while the shortest intervals were for lymphomas (median of 15.8 months) (Fig. 1A).
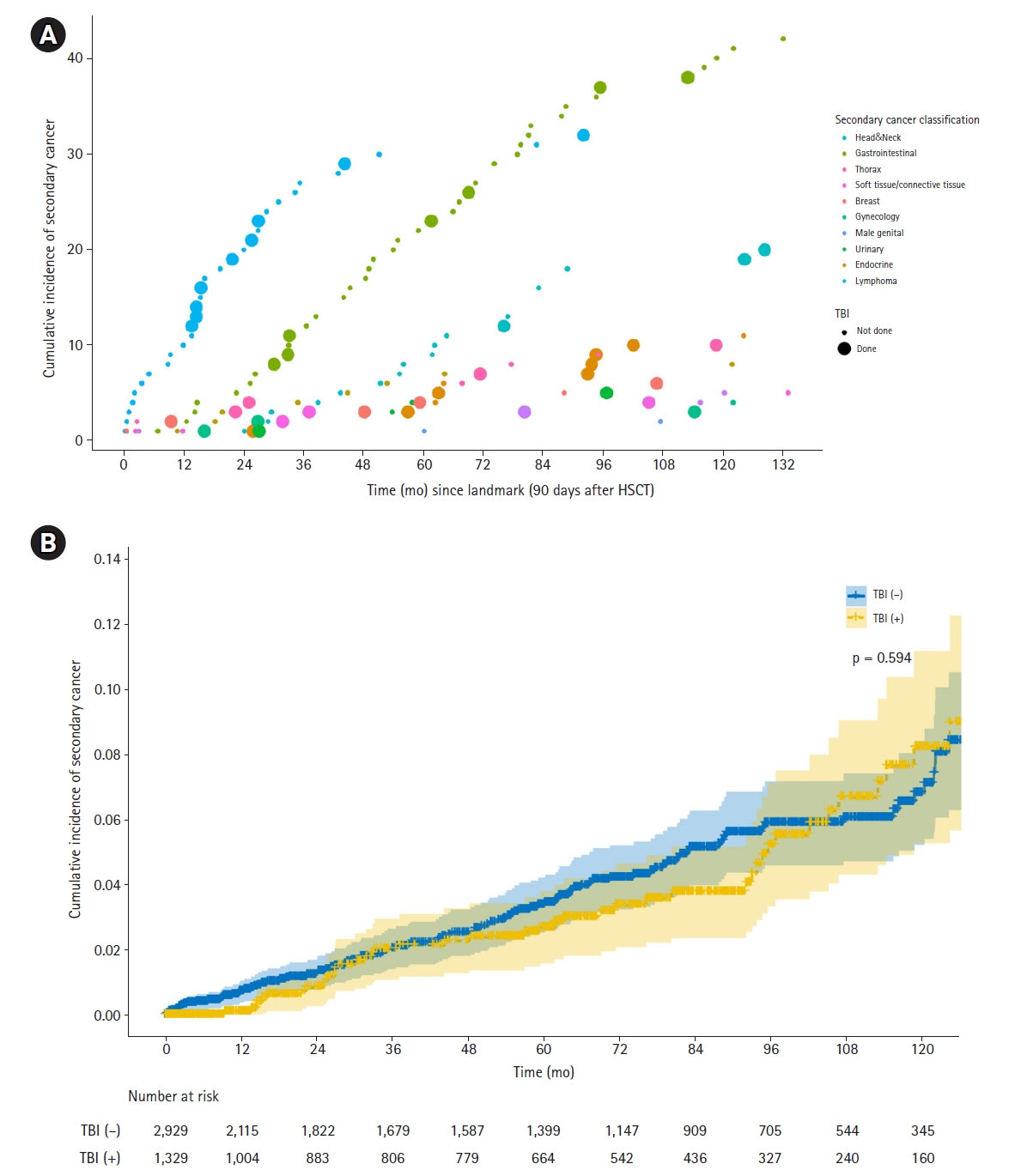
(A) Cumulative incidence of secondary cancers by cancer type depending on whether total body irradiation (TBI) was received after allogeneic hematopoietic stem-cell transplantation in leukemia patients and (B) overall cumulative incidence curve of secondary cancers.
Out of the 143 patients diagnosed with SC, 43 patients had received TBI and 100 patients had not received TBI. The IRs were 6.56 (95% CI, 4.8–8.8) and 7.23 (95% CI, 5.9–8.8) for the TBI and no-TBI groups, respectively; thus, the IRR was 0.91 (95% CI, 0.6–1.3), indicating no significant difference.
SC-free survival analysis indicated that only age was significantly related to subsequent SC occurrence (Tables 2–3) and no significant difference was observed according to TBI status (p = 0.594) (Fig. 1B). In the subgroup analysis according to age group, no differential impact of TBI was observed (Table 4, Supplementary Fig. S2). Even after PSM, age was the sole prognostic factor for poor SC-free survival (p = 0.013), and the IRR of TBI was 1.17 (0.74–1.88) in this group.

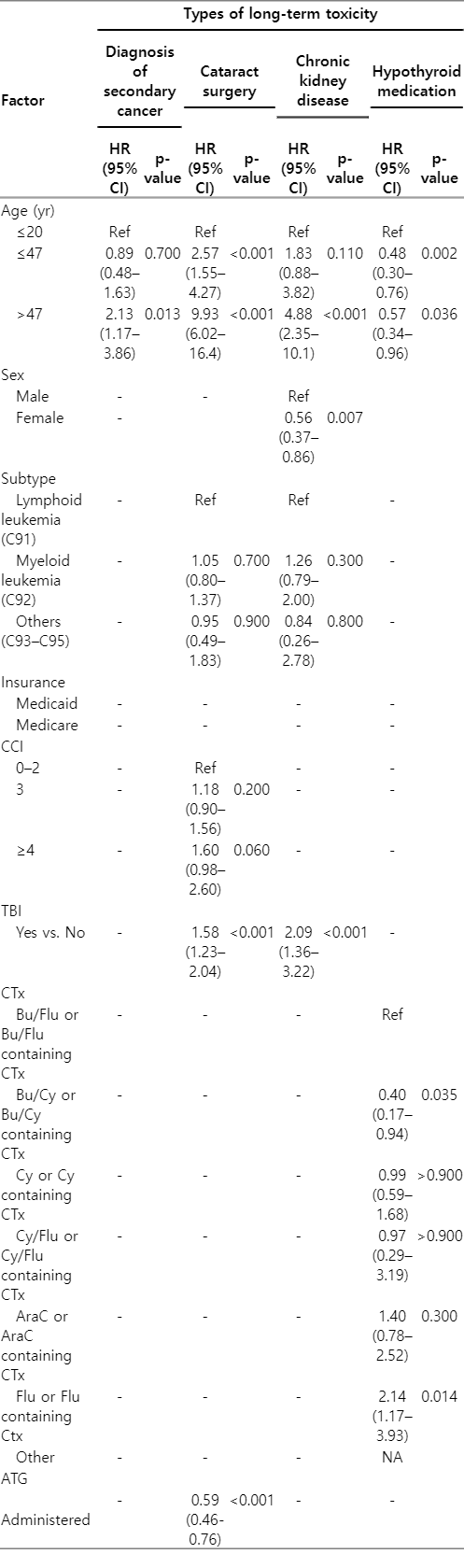
Factors associated with various long-term toxicity-free survival identified by multivariate analysis: in all patients who lived 90 days or more after HSCT
Factors associated with various long-term toxicity-free survival identified by multivariate analysis: in propensity-score matched patients according to TBI who lived 90 days or more after HSCT
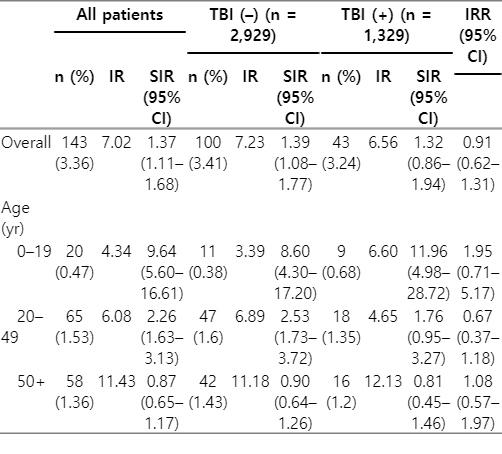
Incidence rate (IR) of secondary cancer after allogeneic hematopoietic stem-cell transplantation (HSCT) with or without TBI and observed standardized incidence ratio (SIR) of secondary cancer matched to general population, analyzed in overall cohort and by age groups
4. SIR of secondary cancer after HSCT
For comparing with general population, we calculated the SIR, and the results are shown in Table 4. After adjusting for age, sex, and year, the SIR in survivors more than 90 days after HSCT was 1.37 (95% CI, 1.1–1.7). The SIR was not significantly increased by TBI (1.32 [0.9–1.9] in the TBI group vs. 1.39 [1.1–1.8] in the no-TBI group). However, it was increased in both groups regardless of TBI in the young age group (0–19 years, SIR 8.60 vs. 11.96; 20–49 years, SIR 2.53 vs. 1.76), while there was no difference compared with the general population for the group over 50 years (SIR was 0.90 vs. 0.81) (Table 4).
5. Cataract after HSCT
The overall incidence of various long-term toxicities after HSCT with or without TBI are summarized in Table 5. Overall, 409 patients underwent cataract surgery for new cataracts after HSCT (crude ratio of 9.6%) with median interval of 33.3 months. The crude ratio of cataract surgery was higher in the TBI group than in the no-TBI group (12.9% vs. 8.1%, p < 0.001). During the observation period, the IR was also higher in the TBI group (28.8 vs. 18.0 cases in the no-TBI group), and the IRR of TBI was 1.60 (95% CI, 1.3–2.0). However, there was no difference in the time interval between HSCT and cataract surgery between the two groups (p = 0.948).
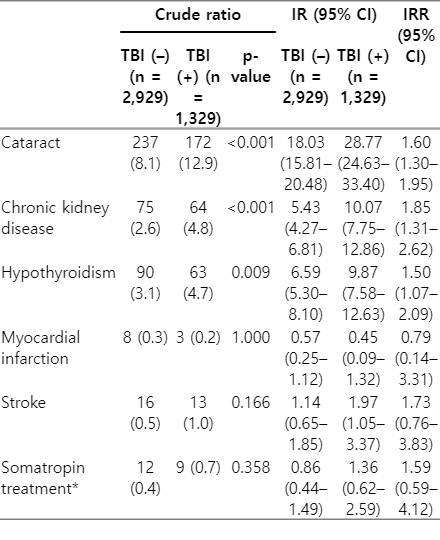
Crude ratio, incidence rate (IR), and incidence rate ratio (IRR) of various long-term toxicities after allogeneic hematopoietic stem-cell transplantation with or without TBI
Multivariate analysis showed that older age, higher CCI scores, and TBI were significant factors related to cataract surgery-free survival (Tables 2–3, Fig. 2A). Multivariate analysis showed similar results between the PSM and pre-matched cohorts (age, CCI scores, and TBI), and the IR of cataract surgery also increased after TBI (17.08 [13.9–20.8] vs. 29.55 [25.3–34.4], respectively; IRR 1.73 [1.3–2.2]).

Cumulative incidence curves of (A) cataracts, (B) chronic kidney disease, and (C) hypothyroidism after allogeneic hematopoietic stem-cell transplantation in leukemia patients. TBI, total body irradiation.
6. CKD after HSCT
During the follow-up period, 139 patients (3.3%) were diagnosed with CKD. The incidence was higher in the TBI group (4.8% vs. 2.6%, p < 0.001) (Table 5). The median time to diagnosis of CKD was 34.2 months; in the TBI group, it was 26.6 months, which was shorter than that in the no-TBI group (median 46.5 months, p = 0.061). The IRs were 5.43 (95% CI, 4.3–6.8) and 10.07 (95% CI, 7.8–12.9) in the no-TBI and TBI groups, respectively, and the IRR was 1.85 (95% CI, 1.3–2.6), indicating more patients developed CKD after TBI. The impact on CKD was particularly pronounced in older patients (IRR 1.03, 1.58, and 2.75 in patients <20 years, 20–47 years, and ≥47 years, respectively).
Multivariate analysis indicated that patient older age, female, insurance type (Medicare), and TBI (Tables 2–3, Fig. 2B) were significant prognosticators impacting CKD-free survival. Similar results were found in the PSM cohort (p < 0.001), with the IRR of TBI was 2.08 (95% CI, 1.3–3.3).
7. Hypothyroidism after HSCT
A total of 153 patients (3.6%) started taking medication for hypothyroidism following HSCT with a median 36 months afterwards. The crude ratio was higher in the TBI group (4.7%) than in the no-TBI group (3.1%, p = 0.009) (Table 5), and there was no difference in time between HSCT and the prescription of medication between the groups (p = 0.658). The IR was 9.87 in the TBI group and 6.59 in the no-TBI group, and the IRR of TBI was 1.50 (95% CI, 1.1–2.1), suggesting that hypothyroidism occurs more often in the TBI group (Table 5). When analyzed based on age, IRR of TBI was higher in older patients (2.29 [1.1–4.6] in patients >47 years old vs. 1.24 [0.7–2.2] in patients ≤20 years old vs. 1.44 [0.8–2.5] in patients 20–47 years old).
An analysis of hypothyroidism medication-free survival indicated that worse outcomes occurred in younger patients and females. Univariate analysis determined that TBI was a significant factor (p = 0.014), but multivariate analysis did not (HR = 1.42, p = 0.130) (Tables 2–3, Fig. 2C).
In the PSM cohort, the IRs were 9.87 (95% CI, 7.5–12.6) and 7.25 (95% CI, 5.3–9.7), respectively, for patients receiving TBI or none, and the IRR of TBI was 1.35 (95% CI, 0.9–2.0). Multivariate analysis also indicated that young age was the most important prognosticator of hypothyroidism medication-free survival (Tables 2–3).
8. MI, stroke, or somatropin treatment after HSCT
We also tried to evaluate whether the incidence of MI or stroke increased after HSCT according to the application of TBI. However, these toxicities were rare; less than 1% of the overall cohort—MI 11 cases (0.3%) and stroke 29 cases (0.7%). There was no significant difference in the frequencies of MI and stroke according to TBI (p = 1.000 and p = 0.166, respectively). For stroke, the IR seemed to slightly increase with TBI, but the IRR was 1.73 (95% CI, 0.8–3.8), which was not significant (Table 5). The analysis by age group showed IRR for stroke was as follows: IRR 7.72 (95% CI, 1.5–74.6) in patients ≤47 years old and IRR 0.98 (95% CI, 0.3–2.9) in patients >47 years old.
Among 884 patients under the age of 20 at the time of HSCT, 20 patients were treated with somatropin after a median of 38 months. The crude ratio according to TBI was not significantly different (2.8% in the TBI group vs. 2.1% in the no-TBI group, p = 0.703), but somatropin treatment was administered earlier after HSCT in the TBI group (median 23.6 months; 53.5 months in the no-TBI group; p = 0.030). In entire cohort, The IRR of TBI was 1.59 (95% CI, 0.6–4.1).
The results of each toxicity-free survival analysis are presented in Supplementary Table S4. Briefly, male patients tended to experience MI more frequently (p = 0.084 in univariate analysis), stroke was common in older patients, and treatment with somatropin was common in younger patients. The increased occurrence of these toxicities due to TBI was unclear (Supplementary Fig. S3).
Discussion and Conclusion
In this work, we investigated the long-term toxicity of TBI in 4,554 leukemic patients who underwent allogeneic HSCT. Overall TRM was 5.8% which was acceptably low compared to previous report using TBI (up to 38%) [15]. After a median follow-up of 5 years, 3.36% of patients experienced subsequent SC, and the risk of SC was higher than that in the general population (SIR 1.37; 95% CI, 1.1–1.7), although it is not possible to determine whether these SC cases are HSCT-induced or de novo second primary. Old age was the most related factor to the occurrence of SC, the SIR showed that cancer incidence did not increase in patients aged 50 years or older compared with the general population (SIR 0.87; 95% CI, 0.7–1.2); instead, the risk of cancer increased in patients aged 20–49 years (SIR 2.26; 95% CI, 1.6–3.1) and under 20 (SIR 9.64; 95% CI, 5.6–16.6). Also, there was no significant increase in cancer incidence according to TBI regardless of age within the present cohort (IRR of TBI, 0.91; 95% CI, 0.6–1.3). For other toxicities, the incidence of cataracts and CKD increased with TBI (cataracts IRR 1.60; CKD IRR 1.85) as well as with age; hypothyroidism was also increased in patients with TBI (IRR 1.50; 95% CI, 1.1–2.1) and especially in younger patients.
Although it has been reported variously, like the results of this study, SC incidence appears to increase after HSCT. St. Jude Children's Research Hospital's retrospective study of 2,169 patients with acute lymphoblastic leukemia treated between 1962 and 1998 reported that the cumulative incidence of SC was 4.17% at 15 years and obviously with an increased overall risk compared with the general population [16]. In another large cohort of 3,182 children diagnosed with acute leukemia who received allogeneic HSCT between 1964 and 1992 at 235 centers in Europe, 25 solid tumors were observed compared with an expected incidence of one case (p < 0.001) [17]. Theoretically, TBI is considered to further increase SC incidence, but it is unclear how much TBI implementation prior to HSCT actually contributes actually to SC development. Baker et al. [6] and Socie et al. [17] showed that high-dose TBI (≥6 Gy) was significantly associated with an increased risk of SC, and the study of Baker et al. [6] focused specifically on the effect of TBI dose and fractionation and confirmed the comparable incidence of SC after low-dose TBI (2–4.5 Gy) of a myeloablative CTx-alone group. In this study, the risk of SC was not further increased in the TBI group compared with the CTx-alone group. Multivariate analysis showed that age was the most important factor contributing to SC-free survival. Subgroup analysis according to age revealed an increased SIR in young patients (<20 years old) compared with that of the CTx-alone group (SIR 8.60 vs. 11.96). This suggests that young patients are more sensitive to radiotherapy, and that an additive effect, resulting from the combination with CTx, may contribute to the occurrence SCs. However, in older patients, the above effects were not identified. Therefore, to minimize the occurrence of SC, it is necessary to consider the patient’s age, and if possible, the use of low-dose or fractionated TBI.
Cataract is one of the most commonly reported long-term toxicities, which is consistent with our study results; the IR per 1,000 person-year increased due to TBI from 18.0 in the CTx-alone group to 28.8 in the TBI group. In addition to TBI, multivariate analysis identified old age and comorbid diseases as significant factors. Gruen et al. [2] investigated the long-term outcomes, toxicities, and occurrences of SC in 109 pediatric leukemia patients. They discovered that 47 patients (43%) experienced long-term toxicities, including abnormal kidney function (6%), hypothyroidism (6%), and cataracts (3%). The observed discrepancy in cataract incidence may be explained by differences in patient populations. In our subgroup analysis of age, cataracts were noted in 2.6% of patients <20 years old and 17.4% of patients >47 years old. However, even in younger patients, the incidence of cataracts increased significantly after TBI (IRR 1.89; 95% CI, 1.5–2.5; data not shown). In a study by Pearlman et al. [7], who analyzed 705 patients who underwent TBI, the median patient age was 57.5 years, and cataracts developed in 16% of patients, similar to the results of our study. The median time between HSCT and cataract development was 3–4 years; this is also consistent with previous reports. The risk of cataract occurrence after TBI is thought to be affected by factors such as dose, fractionation, or regimen. Although study results vary, fractionation appears to lower the risk of cataracts in general. Benyunes et al. [18] showed that fractionated TBI decreases the rate of cataract development from >90% to 30% at 3 years when compared with a single, 10-Gy dose of TBI. A proportional hazards regression model identified single-dose TBI as one of the variables correlated with an increased probability of cataracts (relative risk of 2.46).
Kidney injury remains a serious complication that lowers the survival rate and quality of life after HSCT. CKD, defined as a decrease in the glomerular filtration rate (GFR) below 60 mL/min/m2 lasting more than 3 months, occurs in 5%–11% within about 5 years after HSCT, and 7% of cases proceed to end-stage renal failure [19,20]. GFRs were lower in patients with hematological malignancies than in those without malignant disease [20]. Moreover, TBI is considered the most important risk factor for CKD, and a systematic review by Kal et al. [21] showed the dose–effect relationship between TBI and CKD. Our study also found that TBI increased the incidence of CKD compared with the CTx-alone group (IRR 1.85), especially in elderly patients (IRR 2.75 in patients ≥47 years old).
Thyroid dysfunction, including severe primary hypothyroidism, has been reported in up to 20% of patients treated with bone marrow transplantation without TBI [22]. However, TBI, especially in childhood, is an important prognosticator for thyroid dysfunction, and primary hypothyroidism is the most frequently reported benign thyroid dysfunction following TBI in childhood, ranging from 26% to 50% [23,24]. To overcome the limitations of the database that did not allow review of patients' raw medical records, we defined hypothyroidism as being prescribed drugs for the condition for more than 3 months, and the crude ratio was 3.6%. Ishiguro et al. [23] reported five cases of overt hypothyroidism among 147 patients treated with bone marrow transplantation, and the incidence increased by about 30% if subclinical disease was included. Therefore, we anticipate that there are more patients with compensated hypothyroidism in our cohort as in previous reports. Also, our results showed a significant increase in hypothyroidism after TBI compared with the CTx-only group as for the other toxicities described above, and young age was significantly related to hypothyroid-medication-free survival. However, the IRR of TBI was higher in older patients, which suggests that the impact of TBI could be greater in elderly patients, and regular thyroid function surveillance could be required.
We also evaluated other complications including MI, stroke, and somatropin treatment after HSCT with or without TBI, but few patients experienced these toxicities, and there were no significant differences between groups. However, although the reliability is low due to the small number of toxicity events, the IRR for stroke was increased after TBI in patients ≤47 years. Because the follow-up period of this study was not long enough, there may be differences between groups after sufficient follow-ups, in accordance with recent reviews that described a potential higher risk for stroke in older-aged patients after a TBI-conditioning regimen [25].
Although TBI was verified for improving survival by the FORUM trial and is a mandatory component in some leukemic patients [26], TBI after allogeneic HSCT is associated with multiple late sequelae, leaving room for improvement. Considering technical improvements in radiotherapy planning and delivery, highly conformal TBI or total marrow irradiation, and total marrow and lymphoid irradiation have been investigated to reduce TBI-related toxicities without compromising efficacy. Recently, TBI using intensity-modulated radiotherapy [27] and low-dose TBI [28], which are not discussed in this study, have been associated with favorable treatment outcomes. Therefore, further research will be required after the modern treatment techniques have been adopted in clinical practice.
This study has several limitations. First, the follow-up period of median 5 years was not long enough. Hijiya et al. [16] showed that SC incidence may increase steadily over the 30 years following treatment of acute lymphoblastic leukemia. Therefore, a long-term follow-up study for the patient cohort included in this work should be supported in the future. However, to the best of our knowledge, since we included the largest number of patients ever reported as well as relatively homogeneous group consisting of 4,554 leukemia patients treated within compact period, the data described above also have important value in addition to the existing literature. Second, this study shows the inevitable heterogeneity of cohorts created in a database study. Our cohort contains both lymphoid and myeloid leukemic diseases receiving allogeneic HSCT. Heterogeneity of the TBI conditioning regimens, dose intensities, and application policies between treatment centers was considerable; therefore, we have tried to mitigate this effect through multivariate analysis or PSM analysis, but some degree of heterogeneity remained. Lastly, TBI dose/fractionation effects cannot be analyzed. In contrast to drug prescriptions, radiotherapy claims are based on the number of treatments; thus, the fraction number of TBI can be determined, but the exact dose per fraction cannot.
In conclusion, our results suggest that modern TBI may not additionally increase the risk of SC after allogeneic HSCT, although increased risks of other disease were noted. Moreover, exploratory analysis showed that age was an important factor in predicting various long-term toxicity-free survivals. Physicians should carefully consider individualized risks and benefits of TBI, especially according to age group. Further studies with long-term follow-ups are needed to confirm our findings. Moreover, a deep understanding of other possible long-term toxicities following TBI not covered in this study is also needed.
Notes
Statement of Ethics
This work was performed according to the principles of the Declaration of Helsinki after obtaining approval of the Institutional Review Board of Seoul Metropolitan Government–Seoul National University Boramae Medical Center (IRB No. 07-2022-16). The committee granted an informed consent waiver based on the retrospective nature, and anonymity, of the data used in this work.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Funding
This research was supported by Chungnam National University.
Author Contributions
Conceptualization, Kwon J, Kim BH. Investigation and methodology, Kwon J, Kim BH. Project administration, Kwon J, Kim BH. Resources, Kwon J. Supervision, Kim BH. Writing of the original draft, Kwon J. Writing of the review and editing, Kim BH. Software, Kwon J. Validation, Kim BH. Formal analysis, Kwon J, Kim BH. Data curation, Kwon J, Kim BH. Visualization, Kim BH. All the authors have proofread the final version.
Data Availability Statement
The data that support the findings of this study are available from Health Insurance Review and Assessment Service (HIRA) of the Republic of Korea, but restrictions apply to the availability of these data, which were used under license for this study, and so are not publicly available. Results of the analyzed data can be provided according to reasonable request.
Supplementary Materials
Supplementary materials can be found via https://doi.org/10.3857/roj.2023.00871.
Cumulative incidence curve of (A) treatment-related mortality within 3 months and (B) overall survival according to whether total body irradiation (TBI) was received after allogeneic hematopoietic stem-cell transplantation in entire patients.
Cumulative incidence curve of secondary cancer in patients (A) ≤20 years of age, (B) aged 21–47 years, and (C) >47 years according to whether total body irradiation (TBI) was received after allogeneic hematopoietic stem-cell transplantation in entire patients.
Cumulative incidence curves of (A) myocardial infarction, (B) stroke, and (C) somatropin treatment whether total body irradiation (TBI) was received after allogeneic hematopoietic stem-cell transplantation in entire patients.
Summarized patient and tumor characteristics of the entire cohort
Univariate and multivariate survival analyses in patients treated with hematopoietic stem cell transplantation
Secondary cancer classifications according to ICD-10 codes
Factors associated with long-term toxicity-free survival identified by multivariate analysis (myocardial infarction, stroke, and somatropin treatment)